


Should You Have Surgery Or TAVI If You Have Aortic Valve Stenosis?

Background
One of the commonest questions that patients ask our doctors in clinic is whether surgical replacement of their diseased aortic valve or TAVI is better for them. The answer to this question does not have to be complicated once you understand the subtle difference between the two.
In this short article, we will explain what aortic valve stenosis means, and why it is so important to treat when it becomes severe and causes symptoms. We will then explain the differences between surgical replacement of the aortic valve versus TAVI (transcatheter aortic valve implantation-insertion of a new aortic valve over a wire in the groin).
Aortic Valve Stenosis
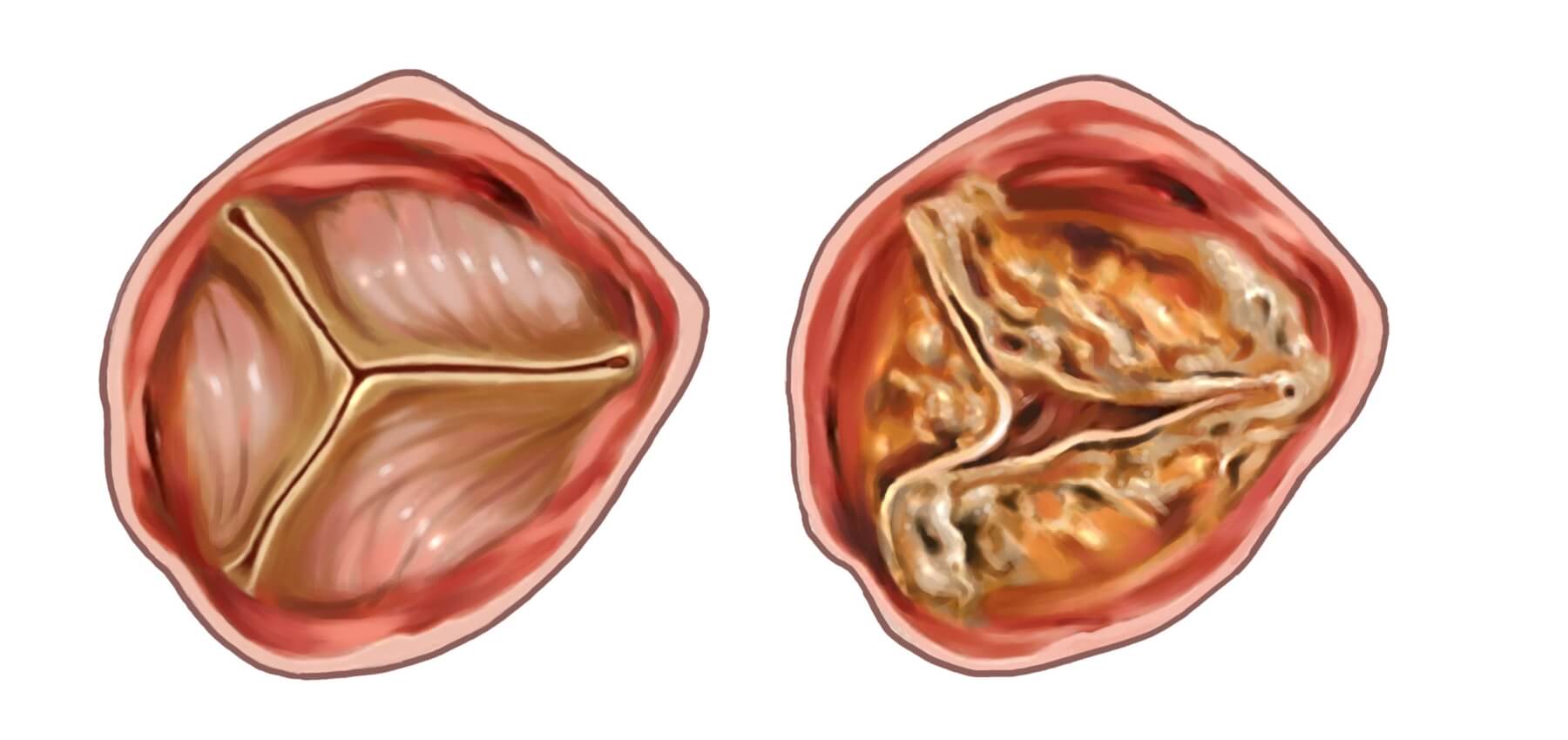
The aortic valve is the last valve in the heart through which blood passes on its way to the body. Aortic valve stenosis is a progressive condition in which the aortic valve leaflets become calcified and rigid. As the stenosis worsens, the heart thickens up to try and force blood through the narrowed valve. Eventually, despite its best efforts, the heart cannot pump enough blood around the body to maintain anything other than restricted activities. Ultimately, this condition is rapidly fatal without rapid treatment. Once a patient starts to experience shortness of breath, dizziness, or chest pain, they only have a 50:50 chance of being alive in 2 years! Fortunately, with treatment, this risk can be removed completely.
Medical treatment for severe symptomatic aortic valve stenosis simply does not work. You need relief of the stenosis by one means or another.
Aortic Valve Surgery
Surgery for aortic stenosis remains the gold standard treatment for aortic valve stenosis. During this treatment, the surgeon performs an operation to cut out the old calcified valve, and to replace it with a new valve made of metal, carbon or animal tissue (pigs or cows valve).
These days, the majority of patients can have this procedure performed without the need for opening the breastbone in a procedure called Anterior Right Thoracotomy Aortic Valve Replacement (ARTAVR). We perform this operation routinely in patients with aortic stenosis because of the much swifter healing (days rather than months), reduced risk of pain, infection and bleeding, and the far superior cosmetic results.
In this treatment, the patient needs a general anaesthetic and we use a heart lung machine to allow us to remove the old valve carefully. We do this through a small cut between the ribs on the right side of the chest rather than through a big sternum cut. Once the old valve is removed, the surgeon can insert a large new valve into the heart very accurately under direct vision. The types of valve that the surgeon uses to replace the aortic valve have received many decades of study. This means that the surgeon is able to precisely predict the long-term durability of the new valve. If you choose a mechanical or carbon valve, these will last a life-time but you will be required to take a blood thinner called Warfarin forever. Tissue valves do not require Warfarin and over the age of 70 years, these valves have an extremely good long-term durability.
Since the surgeon removes the old diseased aortic valve, there is low risk of injury to the electrical system of the heart and the incidence of pacemaker and leaks around the new valve are very low indeed.
TAVI
TAVI is a treatment in which the surgeon inserts the new aortic valve into the heart over a wire inserted in the groin. In this treatment, the old valve is not removed, and there is no need for general anaesthesia or the heart lung machine. The new valve is inserted into the calcified and diseased aortic valve and expanded. This pushes the diseased valve into the neighbouring soft tissues of the heart. This technique has two main limitations:
- The diseased aortic valve is forced into the neighbouring tissues. This results in a much higher risk of injury to the electrical system of the heart, and the resulting need for a pacemaker compared with surgical replacement of the aortic valve.
- The seal between the diseased aortic valve and the new TAVI valve is not always complete and the risk of leaks around the TAVI valve is much higher than with surgical replacement. If this is anything more than mild, then revision of the treatment by surgery may be required.
Other drawbacks relate to the TAVI valve itself. TAVI valve durability is still do not fully understand. Presently, surgical tissue valves offer more predictable long-term durability. TAVI is also not suitable for every disease type (e.g. bicuspid aortic valve, aortic valve regurgitation). Finally, TAVI valves are only made from animal tissues and if you are young and prefer a mechanical valve because of its lifetime durability, then TAVI is not suitable for you.
These limitations mean that TAVI is best suited only for those patients who may not be suitable for surgical replacement on the basis of risk. These risks may include advancing age, severe lung problems, kidney impairment and previous heart surgery amongst others. TAVI is also proving to be useful in patient who have undergone previous aortic valve replacement with a tissue valve which has started to fail.
Our View
The team at The Keyhole Heart Clinic believe that both ARTAVR and TAVI are extremely valuable treatments for patients with aortic valve stenosis. Our current treatment preference is to assess patients for minimally invasive surgical aortic valve replacement using the ARTAVR technique. If patients are found to be too risky for this procedure, then TAVI is offered as long as the patient understands the benefits and limitations of this procedure.

