


CT Coronary Angiography: A Key to Early Heart Disease Screening in the UK

Heart disease is a major concern for many people over 40, especially those with risk factors or a family history. In the UK, heart disease screening often starts with lifestyle assessment and basic tests, but advanced imaging is transforming how we detect problems early. One such tool is CT coronary angiography (CTCA) – a specialised heart CT scan that can spot signs of coronary artery disease before symptoms worsen. This article explains what CTCA scans are, how they work, who they’re for, and why they add value in heart disease screening in the UK. We’ll also compare CTCA to other tests (like ECGs and stress tests), discuss its role in NHS and private care (including private heart scans in London), outline what to expect during a scan, and weigh the benefits and limitations. Our goal is to provide trustworthy, reassuring information on CTCA and early detection of heart disease, on behalf of The Keyhole Heart Clinic.
What Is CT Coronary Angiography (CTCA)?
CT coronary angiography is a non-invasive medical imaging test that visualises the heart’s arteries (the coronary arteries) using a powerful X-ray CT scanner. “Non-invasive” means no surgical instruments are placed inside the body. During a CTCA, an iodine-based contrast dye is injected into your bloodstream through a small vein (usually in the arm). As your heart is scanned, the dye highlights the coronary arteries, allowing doctors to see detailed 3D images of blood flow and any coronary artery disease (such as fatty plaques or narrowings). The CT scanner is a doughnut-shaped machine; you lie on a table that slides through it while X-ray images are taken. The process is painless and quick. Because CTCA uses an IV line for dye rather than threading a catheter into the heart, it’s much less invasive than a traditional angiogram procedure. In fact, no recovery time is needed – you can go home shortly after the test.
Despite being less invasive, CTCA produces highly detailed pictures of the coronary arteries. Doctors can identify build-ups of plaque, calcifications, or any blockages that might restrict blood flow to the heart. This is crucial for coronary artery disease diagnosis and screening. If the scan is normal, it provides great reassurance that the heart’s arteries are clear. If problems are seen, you and your doctor can take action early. In technical terms, CTCA has a very high sensitivity (reported around 95–99%) for detecting significant coronary artery blockages, meaning it can reliably find even mild disease. It also has an excellent negative predictive value – if your CTCA is normal, studies show it virtually rules out significant disease, giving you peace of mind. In summary, a CT coronary angiography combines advanced X-ray technology with computer analysis to give a detailed view of your heart’s blood vessels without any incisions.
Who Should Consider a CT Coronary Scan?
Not everyone needs a CTCA; it’s typically recommended for specific groups of patients. UK guidelines now recommend CT coronary angiography as the first-line test for people with new or suspected angina (chest pain due to heart disease) who have no previous diagnosis of coronary disease. In practice, if you visit your GP or a chest pain clinic with symptoms suggestive of angina, you are likely to be referred for a CTCA on the NHS. The scan will show whether any fatty plaques or narrowing exist in your coronary arteries, helping doctors determine if your pain is due to heart disease or not.
Beyond people with chest pain, CTCA can be suitable for those at intermediate or higher risk of heart disease – for example, individuals over 40 with multiple risk factors (like high cholesterol, high blood pressure, or a strong family history). These patients may not have symptoms yet but are anxious about their heart health. For them, a CTCA can be an informative screening tool for early detection of heart disease. Indeed, some health-conscious individuals opt for a private heart scan in London or other UK cities to proactively check their coronary arteries. The Keyhole Heart Clinic and similar specialist centres offer CTCA scans to such patients for peace of mind and early intervention if needed.
However, CTCA is not needed for everyone. If you’re young, have no risk factors, or your calculated risk of heart disease is very low, lifestyle improvements and routine check-ups might be all you need. CTCA also isn’t recommended if you already have a very high probability of significant disease (for instance, classic symptoms in a high-risk person), in which case doctors might proceed directly to treatment or an invasive angiogram. Instead, CTCA is most valuable for those in between – people with some risk or vague symptoms where the scan can clarify things. Always consult a doctor to see if CTCA is appropriate in your case. There are also a few groups who should generally avoid CTCA, such as pregnant women (due to X-ray radiation) and patients with severe kidney impairment or severe contrast dye allergies. The contrast dye contains iodine, so if you’ve had a prior reaction or have uncontrolled asthma, special precautions or alternative tests may be considered. Your healthcare team will screen for these factors to ensure CT scanning is safe for you.
Early Detection of Coronary Artery Disease with CTCA
One of the biggest advantages of CT coronary angiography is its power in early detection of heart disease. Coronary artery disease (CAD) often develops silently over years. Fatty deposits (plaques) can build up in the arteries without causing noticeable symptoms until they become severe. A CTCA can reveal these plaques at an early stage – even if an artery is only partially narrowed or if the plaque is “soft” (not yet calcified). Detecting CAD early means you can take steps to prevent a heart attack or worsening disease. This might include lifestyle changes (diet, exercise, quitting smoking), medications like statins to lower cholesterol, or other preventive therapies. In some cases, if a significant blockage is found, timely referral for treatments like angioplasty (stents) can be made before a heart attack ever occurs.
Research supports the value of CTCA in improving outcomes. A major UK clinical trial called SCOT-HEART studied patients with chest pain and found that adding CT coronary angiography to standard care significantly reduced heart attacks and heart disease deaths over the following years. In fact, over 5 years, the group who had CT scans had about a 40% lower rate of heart attack or coronary death compared to those who only had routine tests. This benefit came without a big increase in invasive procedures; in other words, CTCA helped guide better preventive care and targeted treatment for those who needed it. The lesson is clear – knowing about plaque in your arteries sooner rather than later can be a lifesaver. It allows doctors and patients to make informed decisions to manage the condition early on. Even for asymptomatic individuals, a CTCA that shows mild disease can serve as a wake-up call to intensify healthy habits and medications to halt progression of coronary disease.
Equally important, if your CTCA is completely normal, that provides immediate reassurance. You can be confident you’re not currently at high risk of a heart attack from a blocked artery. For an anxious patient, this peace of mind is invaluable. Many experts note that CTCA’s greatest strength is its ability to exclude significant coronary disease when the scan is normal. In summary, CT coronary angiography offers an accurate early look at coronary artery health, empowering you to take action and potentially avoid future heart problems.
CTCA vs Other Heart Screening Tests
How does CT coronary angiography compare to more traditional heart tests? Each test has a role, but CTCA offers a unique combination of non-invasiveness and detailed imaging. Below is a comparison of CTCA with other common screening tools:
- Resting Electrocardiogram (ECG): An ECG records the electrical activity of your heart via sticky patches on the skin. It’s a simple and widely available test that can detect rhythm problems or signs of a past heart attack. However, as a screening tool for coronary artery blockages, a resting ECG is limited. Many people with early or even moderate coronary disease will have a completely normal ECG at rest. It mainly helps if damage has already occurred or if there are ongoing rhythm issues, but it cannot visualize the arteries or detect plaques. So while an ECG is an important basic test, a normal result doesn’t rule out heart disease if risk is present.
- Exercise Stress Test (Treadmill ECG): This involves recording the ECG while you exercise (usually on a treadmill or bike) to see if exertion causes any ECG changes suggestive of reduced blood flow to the heart. Stress tests have been used for decades to screen for significant coronary disease. They are non-invasive and can indicate if an artery narrowing is causing ischemia (lack of oxygen) under stress. The downside: stress tests are not very sensitive for early or mild disease. They typically only turn positive when an artery is quite narrowed (often >70%) and causing reduced blood supply. Even then, the accuracy varies – standard exercise ECGs detect roughly only about 2 out of 3 cases of significant disease (around 68% sensitivity). CTCA, by contrast, directly visualises even modest plaques and has much higher sensitivity and detail. Also, some people cannot exercise well due to arthritis, lung issues, etc., limiting the usefulness of a treadmill test. In short, a stress ECG is a good functional test, but it can miss early disease. CTCA can complement or replace it in many scenarios by providing an anatomical map of any blockages.
- Echocardiogram (Heart Ultrasound) and Stress Echo: An echocardiogram uses ultrasound waves to create images of the heart’s structure and pumping function. It’s great for checking heart muscle strength, valves, and other conditions, but it doesn’t show the coronary arteries. A stress echocardiogram combines ultrasound with exercise or medication-induced stress to see if parts of the heart wall move abnormally (indicating poor blood flow). Stress echos can detect significant coronary disease (with good specificity), but like treadmill tests, they may not catch smaller plaques that aren’t yet causing wall motion changes. They also require an expert and image quality can be affected by body shape or lung interference. CTCA, by directly showing the arteries, can find disease before it ever causes an echo change.
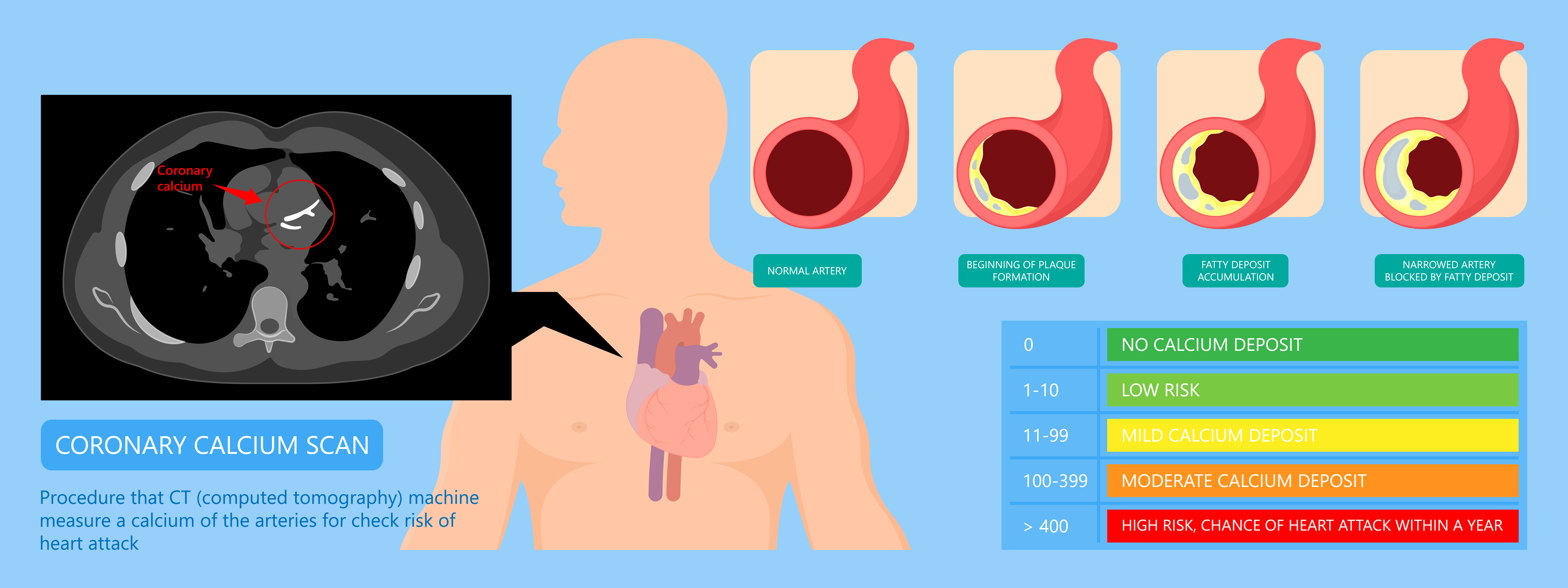
- CT Calcium Scoring: This is a simpler form of CT scan (no dye injection) that measures calcified plaque in the coronary arteries. You receive a “calcium score” – a number reflecting how much hard plaque you have. A score of zero is reassuring (no calcified plaque), whereas higher scores mean more plaque and higher risk. Calcium scoring is a useful screening tool, especially for asymptomatic people around 40-70 years old who want to refine their risk assessment. It’s quick, with very low radiation, and if the score is zero, your 5-year risk of a heart attack is extremely low. However, a calcium scan doesn’t show actual artery narrowings or soft (non-calcified) plaque. It merely quantifies calcification. Also, if the score is above zero, you might still need further tests. In fact, in many cases a CTCA is the next step if a calcium score is elevated. CTCA includes information about soft plaque and the degree of any blockage, which calcium scoring alone cannot provide. So calcium scoring can be a good first check for some; CTCA is more comprehensive if detailed info is needed.
- Invasive Coronary Angiography: Often just called an angiogram, this is the traditional test where a catheter is inserted (via wrist or groin) into the heart’s arteries and dye is injected while X-ray videos are taken. It’s the gold-standard test for diagnosing coronary artery disease because it provides very clear images and allows treatment (like stents) at the same time if needed. The downside is that it’s an invasive procedure – you need local anaesthesia, there’s a small risk of complications (bleeding, artery damage, etc.), and it requires recovery time. CTCA was developed as a non-invasive alternative to get much of the same information without those risks. For most patients in a screening or diagnostic scenario, CTCA is preferred initially. If the CTCA results show severe blockage, you may then be referred for an invasive angiogram to confirm and possibly treat it. It’s worth noting that CTCA is extremely good for medium-to-large coronary arteries; however, it may be less reliable in very small vessels or intricate branch arteries. In such tiny vessels, even a traditional angiogram can be challenging, but it’s still considered the definitive test. Overall, for most people, CTCA provides a nearly equivalent view to an invasive angiogram for diagnostic purposes – with far fewer risks. In fact, invasive angiograms are now often reserved for when intervention is likely needed, thanks to CTCA’s capabilities.
In summary, CT coronary angiography stands out by combining the clarity of an anatomic test (like an invasive angiogram) with the safety and convenience of a non-invasive test. It outperforms basic screening methods (ECG, exercise tests) in detecting disease, and is often used alongside or before invasive procedures. This is why UK cardiology guidelines have shifted to use CTCA early in the pathway for diagnosing coronary artery disease.
CTCA in the UK: NHS Pathways and Private Options
In the United Kingdom, the use of CT coronary angiography has grown significantly in recent years. On the NHS, CTCA is now embedded in the care pathway for patients with suspected angina. If you see a cardiologist or attend a rapid access chest pain clinic, and you do not already have a diagnosis of coronary disease, a CTCA is likely to be the first major test you undergo. NHS England has invested in modern 64-slice (and higher) CT scanners across the country to facilitate this service. In some cases, the NHS is also using advanced software (such as HeartFlow analysis) which can take CTCA images and further analyse blood flow, but the core of the process is the CT scan itself. Generally, an NHS-referred CTCA for chest pain will be free at the point of use, but there may be waiting lists due to demand.
For patients who don’t have typical angina symptoms but are simply concerned about their heart risk, accessing CTCA through the NHS can be more challenging. The NHS tends to reserve CT scans for those meeting certain clinical criteria (because of cost and resource limitations, and to avoid unnecessary radiation exposure in low-risk individuals). If you have risk factors and anxiety but no clear symptoms, your GP might first perform a risk assessment (blood tests, blood pressure, etc.) as part of an NHS Health Check. They might then decide if a referral to a cardiologist is warranted. In many cases, purely for screening without symptoms, the NHS will focus on risk factor management (e.g. advising diet, exercise, medications) rather than immediately doing a CT scan.
This is where private heart scan options come in. In the private healthcare sector, patients have more flexibility to request advanced screening tests. Private CTCA scans in London and other major cities are offered by specialist clinics and hospitals. The Keyhole Heart Clinic, for example, provides CT coronary angiography for patients who want a thorough evaluation of their coronary arteries, often without needing a GP referral. The benefits of going private include shorter waiting times and the ability to have the scan even if you have borderline indications. Many patients who are otherwise healthy but have a family history of heart disease choose this route for peace of mind. A CTCA scan in London privately typically involves an initial consultation, the scan itself, and a follow-up to explain results. Private providers ensure that proper safety protocols are followed and that the scan is justified – they will still assess your history and might suggest a calcium score first if appropriate. Do note that private CTCA is an out-of-pocket expense (unless covered by certain insurance plans) and costs can range in the hundreds of pounds. It’s wise to discuss the necessity and benefit with a cardiologist so you make an informed choice.
In both NHS and private settings, CTCA has become a bridge between basic risk evaluation and invasive procedures. Its adoption in the UK reflects a commitment to early, accurate detection of heart disease. Patients should feel reassured that this technology is available and mature. Whether you access it via the NHS (due to symptoms) or privately (for screening and reassurance), CTCA can be a cornerstone of heart disease screening in the UK, especially for those in midlife and beyond with concerns about heart health.
What to Expect During a CTCA Scan
It’s normal to feel a bit nervous if you’ve never had a CT scan before. Knowing what will happen can ease anxiety. Here’s a step-by-step look at what patients can expect during a CT coronary angiography:
A patient being prepared for a CT coronary angiography scan. The CT scanner’s doughnut-shaped opening and the sliding table can be seen, illustrating the non-invasive nature of this heart scan.
- Before the Scan – Preparation: In the days leading up to your CTCA, you’ll receive instructions on preparing. Typically, you should avoid caffeine (coffee, tea, energy drinks) for at least 12 hours before the scan. Caffeine can increase your heart rate, and a slower heart rate yields clearer images. You’ll also likely be asked to have nothing to eat for about 4–8 hours before the scan. Drinking water is encouraged to keep you hydrated, but you should avoid heavy meals. If you take certain medications, your doctor might advise adjusting the timing on the day of the test (always confirm with them). Wear comfortable clothing and avoid metallic items like jewellery or underwire bras; you’ll usually change into a hospital gown for the scan.
- On Arrival at the Clinic/Hospital: You’ll check in and a radiographer or cardiac nurse will meet you to go over the process. They’ll ask some safety questions (confirming no allergies, not pregnant, etc.) and have you sign a consent form. They will take your blood pressure and may check your heart rate. If your pulse is too fast (typically above ~60-70 beats per minute), you might be given a beta-blocker medication to slow your heart rate. This can be given as a pill or through an IV and helps ensure the images aren’t blurry. Some centres also give a dose of nitroglycerin spray under the tongue just before scanning – this temporarily widens the coronary arteries for even better imaging detail. Next, an IV line will be inserted in your arm. Through this IV the contrast dye will be injected later during the scan. Sticky electrode patches will be placed on your chest to monitor your heart rhythm during the test.
- The Scanning Procedure: You’ll be helped onto the CT scanner table, lying flat on your back. The table will slide into the scanner’s circular gantry, which is open at both ends (not a long tunnel like an MRI, so it’s generally well tolerated even by those who dislike tight spaces). The staff will ensure you’re comfortable – you might have a pillow under your head and straps or foam pads to help you stay still. It’s very important not to move during the short scan. The technologist will likely step into an adjacent control room (visible through a window) to operate the scanner, but they’ll stay in contact via intercom. You’ll hear whirring sounds as the CT machine rotates. Initially, some quick scans are done to plan the study. Then, when it’s time for the main images, the iodine contrast will be injected through your IV. You might feel a warm flush or a metallic taste for a few seconds – this is normal and passes quickly. You will be instructed to hold your breath for a short period (usually around 5–10 seconds) while the images are taken. The actual X-ray scanning only lasts a few seconds to moments; modern CT scanners are incredibly fast – sometimes capturing the heart in just one heartbeat or within a single breath-hold. The table may move in and out a couple of times to get all necessary angles. Throughout, your heart rhythm is monitored, and the scanner is timed with your heartbeat to get clear snapshots between beats.
- After the Scan: Once the imaging is complete, the radiographer will remove the IV and you can sit up. There is no recovery time needed – you won’t feel any after-effects from the scan itself. The only advice is to drink plenty of water over the next day to help flush the contrast dye out of your system a bit faster. In most cases, you can drive yourself home and carry on with your normal routine immediately. The scan images will be processed and later reviewed by a specialist (often a cardiologist or radiologist experienced in cardiac CT). They will interpret the findings – for example, measuring any narrowings or noting any plaques – and generate a report.
Results are usually available fairly quickly, but it might take a short while (perhaps the same day or a few days) for the final report, depending on the clinic. The doctor who requested the scan (or the specialist at the scanning centre) will explain the results to you and discuss next steps. It could be as simple as “Great news – no significant issues found, carry on with healthy habits,” or if something is found, they might recommend treatments or further tests. Remember that having some plaque detected is not uncommon as we age; it doesn’t necessarily mean you’ll need an operation, but it does give valuable information to manage your heart health proactively.
Overall, a CTCA scan is straightforward and typically takes about 30 minutes to an hour in total (including prep time), with the scanning itself only a few minutes. Patients generally find it far easier than they imagined – it’s non-invasive, and aside from the IV and breath-holding, there’s little discomfort. The medical team will be there to answer questions and make you comfortable. If you’re feeling anxious, let them know; sometimes even a mild sedative can be offered, though that’s rarely needed.
Benefits of CT Coronary Angiography
CTCA offers several important benefits for patients concerned about their heart health:
- Early Detection and Prevention: As discussed, CTCA can reveal coronary artery disease at an early stage, enabling early interventions. By identifying plaques or narrowings before they cause a heart attack, you can start treatments or lifestyle changes promptly. This proactive approach can prevent serious events and has been shown to improve long-term outcomes.
- Peace of Mind Through Reassurance: For someone worried about heart disease, a normal CTCA is extremely reassuring. It effectively rules out significant blockages in the coronary arteries. This relief from uncertainty can reduce anxiety and stress. Even if minor plaque is found, knowing about it is better than the fear of the unknown – you have a clear picture of your heart health.
- Informed Decision-Making: CTCA provides detailed information that helps doctors and patients make informed decisions. For example, if moderate plaque is seen, your doctor might decide to start a cholesterol-lowering medication or aspirin to mitigate risk. If a severe narrowing is found, you can be referred for further evaluation or treatment (such as an angiogram and stent) in a timely manner. Conversely, if the scan is clean, you might avoid unnecessary medications or invasive tests. In short, CTCA guides a personalised care plan based on actual imaging evidence of your arteries.
- Non-Invasive Convenience: Unlike conventional coronary angiography, CTCA involves no arterial catheters, no hospital stay, and minimal risk. The scan is done as an outpatient procedure and you can resume normal activities right away. This convenience and safety make it an attractive option for screening and diagnosis. It’s especially valuable for patients who are not keen on undergoing an invasive test unless absolutely necessary.
- Comprehensive View: CTCA not only identifies narrowings but can also give insight into the nature of plaque (calcified vs soft) and the overall condition of your heart and adjacent structures. Sometimes incidental findings (like an early lung issue or aneurysm) might be spotted, which can be helpful information for your overall health (though this is an extra, not the main purpose). The point is that CTCA provides a comprehensive snapshot of your heart’s anatomy in one go.
- Guiding Timely Treatment: By stratifying patients into risk categories, CTCA ensures that those who need aggressive treatment get it on time, and those who don’t can avoid invasive procedures. The SCOT-HEART trial, for instance, demonstrated that using CT scans led to more people being started on preventive therapies and a subsequent drop in heart attacks. Thus, CTCA serves as a guide for timely therapy – whether that’s medication, lifestyle change, or referral for interventions.
In essence, CT coronary angiography empowers patients and doctors with knowledge. Early knowledge of heart disease can save lives, while a clean bill of health from the scan offers relief and confidence. This aligns perfectly with a patient-focused, preventative approach to cardiovascular care.
Limitations and Considerations of CTCA
While CT coronary angiography is a fantastic tool, it’s important to understand its limitations and consider when it’s appropriate. Here are some key points to keep in mind:
- Not a Routine Test for Everyone: CTCA involves exposure to X-ray radiation and use of contrast dye, so it’s not something to do without a good reason. If your risk of heart disease is very low, the potential downsides may outweigh the benefit. Healthcare providers follow guidelines to ensure CTCA is used when it’s likely to provide useful information. For low-risk individuals, controlling risk factors (like diet, exercise, and blood pressure) might be recommended instead of jumping to a scan.
- Radiation Exposure: A CTCA does involve radiation, roughly equivalent to the natural background radiation we all receive over about a year or so. This dose is considered low and generally safe, but it’s not zero. Repeated scans are not advisable unless necessary. That said, technology improvements have lowered CTCA radiation doses significantly over the years. Doctors will only recommend the scan if the potential insight gained is worth this minimal risk. Still, it remains a consideration, especially for younger patients, and why it’s not used indiscriminately.
- Contrast Dye Risks: The iodine contrast used in CTCA is very safe for the vast majority of people. However, a small fraction of patients may experience allergic reactions. Severe reactions are rare, and screening questions are used to identify those at risk (e.g. people who have had a prior contrast allergy). Such patients might require pre-medication or an alternative test. Additionally, if you have significant kidney disease, the contrast could potentially worsen your kidney function. This is usually not a concern unless kidneys are already quite impaired, but it’s part of the reason CTCA might be avoided in patients with advanced kidney failure. Hydration before and after the test helps protect the kidneys, and doctors weigh this risk against the benefits.
- Incidental Findings: Because CTCA captures images of structures around the heart (lungs, portions of the chest, etc.), there is a chance of finding unrelated abnormalities. While this can sometimes be beneficial (early detection of another issue), it can also lead to anxiety or additional tests that turn out to be unnecessary. This isn’t exactly a limitation – more a side effect of any advanced imaging. Radiologists are trained to differentiate significant incidental findings from trivial ones, so it shouldn’t deter you, but be aware that comprehensive scans can uncover unexpected tidbits that might need follow-up.
- May Not Eliminate Need for Further Tests: If CTCA results are unclear or show something concerning, you might still need another test afterwards. For example, if a CTCA finds an ambiguous blockage, your doctor might suggest a stress test or even an invasive angiogram to get more information. Or if severe disease is seen, an angiogram would be the next step to potentially treat it. CTCA is often one part of a diagnostic pathway. The good news is, a normal CTCA usually means no further cardiac tests are needed at that time, and a clearly abnormal CTCA gets you swiftly to the right treatment. Just know that it’s not always the final word – it’s part of the bigger picture of your care.
- Availability and Cost: While widely available, CTCA still requires advanced scanners and expertise. In some regions or smaller hospitals, it might not be immediately accessible. If you go private, the cost of a CTCA scan can be a consideration for some patients, as insurance may or may not cover a screening exam. It’s worth discussing fees upfront if you’re going the private route. On the NHS, availability is increasing, but in areas with longer wait times, you might consider traveling to a centre with faster service or using private facilities if timely screening is crucial to you.
- Patient Factors: Certain factors can affect CTCA image quality. Patients with very fast or irregular heart rhythms (like uncontrolled atrial fibrillation) can be challenging to image – the heart’s motion may blur the pictures. Heavily calcified arteries can sometimes cause “blooming” artifacts on CT that make it tricky to gauge the exact narrowing. In obese patients, image clarity might be reduced, though modern scanners are quite good with adjustments. These aren’t reasons to avoid CTCA outright, but they can limit the test’s diagnostic yield in specific scenarios. Doctors may anticipate these and either prep the patient (using medications to steady heart rate) or choose a different test if CT is deemed not suitable.
To summarise, CTCA is not a one-size-fits-all magic bullet – it has limitations related to radiation, contrast use, and certain technical aspects. But when used appropriately, its benefits far outweigh these considerations. A careful medical evaluation will ensure that you undergo CT coronary angiography only if it’s the right test for you. When in doubt, ask questions about why the scan is or isn’t recommended in your situation.
Frequently Asked Questions (FAQ) about CT Coronary Angiography
Q: Is CT coronary angiography safe?
A: Yes, CTCA is considered very safe. The procedure is non-invasive and complications are extremely rare. The main safety aspects – radiation and contrast dye – are managed carefully. The radiation dose is kept as low as possible and is comparable to natural background levels over a year. The contrast dye can, in rare cases, cause allergic reactions or affect the kidneys, but you will be screened for risk factors beforehand. Overall, for the vast majority of patients, the risk associated with CTCA is minimal, especially when weighed against the valuable information it provides. If you have specific concerns (e.g., past contrast reaction or pregnancy), your doctor will address those and might suggest alternative strategies or pre-medication to ensure safety.
Q: How long does a CTCA scan take and will I get results immediately?
A: The CT scan itself is very fast – often just a few seconds of scanning, plus some preparation time. In total, expect to be at the clinic or hospital for around an hour. This includes the prep (paperwork, IV insertion, possibly medication to slow the heart), the actual scan, and a short observation or wrap-up period afterwards. You won’t receive a detailed result on the spot because the scan images need to be processed and reviewed by a specialist. In some cases, the clinician performing the scan might give you a brief initial impression (“the images look okay” or “there might be some blockage we’ll analyze further”). But the formal report usually comes a bit later, often the same day or within a few days, depending on how the service is set up. Your referring doctor will then discuss the results with you and what they mean for your care.
Q: How does CTCA fit into my overall heart disease screening or check-up?
A: CTCA is one component of heart health assessment. It excels at anatomically visualising coronary artery disease. However, it doesn’t replace the need for managing risk factors. Think of it this way: screening for heart disease often starts with evaluating your risk factors (blood pressure, cholesterol, blood sugar, etc.) and lifestyle. If those point to higher risk or if you have worrisome symptoms, CTCA comes in as a detailed diagnostic test to guide next steps. It complements other tests – for instance, you might have a CTCA instead of a stress test as an initial evaluation. Or you might have had a borderline treadmill test and then get a CTCA for clarification. It also complements preventative care: regardless of CTCA results, maintaining a heart-healthy lifestyle is crucial. A normal CTCA isn’t a free pass to neglect diet and exercise (plaques can develop later if risk factors aren’t controlled), and an abnormal CTCA is a call to arms to really double-down on those preventive measures, in addition to any medical treatments. Your healthcare providers will integrate the CTCA findings with the rest of your health profile to create a comprehensive plan.
Q: If CTCA is so good, does it mean I won’t need an angiogram or other tests?
A: In many cases, a CTCA can spare you an invasive angiogram – at least as a first step. If CTCA shows minimal or no blockage, you definitely won’t need an angiogram. If it shows moderate disease, you still might not need an invasive test; you could be managed with medications and lifestyle and monitored over time. If CTCA shows severe disease (for example, a very tight blockage in a main artery), you likely will be referred for a traditional angiogram. The angiogram in that scenario often serves as a prelude to treatment (like inserting a stent) because you wouldn’t do an open-heart surgery or stent based on CT alone without confirmation. So, CTCA can reduce the number of people who undergo angiograms unnecessarily. It triages who actually needs an invasive procedure. Also, sometimes CTCA results will prompt other tests: for instance, if CT shows an intermediate blockage, a doctor might order a perfusion scan or use special CT-based analysis (like FFR-CT or HeartFlow) to see if that blockage is truly causing a blood flow problem. In summary, CTCA often answers the key questions, but it can also indicate when additional tests are or aren’t needed. It’s part of a tailored approach – not always the final step, but a very important one.
Q: Can I get a CTCA scan at The Keyhole Heart Clinic and do I need a referral?
A: The Keyhole Heart Clinic has partnered with the best diagnostic services in London to offer advanced cardiac imaging, including CT coronary angiography, as part of our screening and diagnostic services. One of our goals is to make private heart scans in London accessible to individuals who are concerned about their heart health. You do not always need an external referral – you can contact us directly to discuss your needs. Our team will typically schedule an initial consultation with a cardiologist who will evaluate your risk factors, explain the procedure, and ensure CTCA is the right test for you. If you have recent medical records or test results, it’s useful to share those. We then arrange the CTCA at a partnering state-of-the-art facility. After the scan, our specialists at The Keyhole Heart Clinic will review the results with you in detail and advise you on any further action or preventive measures. We aim to provide a seamless, patient-focused experience – from the moment you inquire about a CTCA scan in London with us, to the follow-up where we plan your path to maintaining a healthy heart.
Conclusion: Taking Charge of Your Heart Health
CT coronary angiography has emerged as a valuable tool in the fight against heart disease. By enabling early detection of coronary artery disease, CTCA empowers patients and doctors to make informed decisions – whether that means getting the all-clear and enjoying peace of mind, or catching a problem early and fixing it before it causes harm. For health-conscious individuals over 40 in the UK, especially those with risk factors or nagging worries, CTCA can provide clarity and reassurance as part of a comprehensive heart screening strategy. It bridges the gap between basic check-ups and more invasive procedures, offering detailed insights non-invasively.
At The Keyhole Heart Clinic, we believe in a trustworthy, patient-centred approach to heart health. Our goal is to inform and reassure, not to alarm. While not everyone needs a high-tech scan, those who do can benefit greatly from the knowledge it provides. If you’re concerned about your risk or have questions about your heart, we encourage you to reach out and discuss whether a CT coronary angiography or another screening option is suitable for you. Early awareness and action are key – with modern tools like CTCA, you have the opportunity to stay one step ahead of heart disease.
Take the next step in looking after your heart. Feel free to contact The Keyhole Heart Clinic to explore your heart screening options – our team is here to guide you with expert advice in a trustworthy, authoritative and empathetic manner. Your heart health is our priority, and together we can ensure you get the best possible care and the peace of mind you deserve.
References:
- British Heart Foundation – Focus on: CT scans of the heart (Heart Matters Magazine, June 2021).
- British Heart Foundation – Coronary Angiogram (BHF patient information page), updated June 2023.
- Matta, M. Stress testing and noninvasive coronary imaging: What’s the best test for my patient? Cleveland Clinic Journal of Medicine, 88(9):502-515 (Sep 2021).
- SCOT-HEART Investigators (Newby DE, et al.). Coronary CT Angiography and 5-Year Risk of Myocardial Infarction. New England Journal of Medicine 379(10):924-933 (2018).
- Mayo Clinic – CT coronary angiogram overview and patient instructions (MayoClinic.org, accessed 2025).

