


Cardiac Myxoma: Benign Heart Tumour. Recovery with Keyhole Treatment.

When you’re told there’s a “tumour in your heart”, it’s almost impossible not to panic.
Most people have never heard of a cardiac myxoma before the day it appears on a scan – and the combination of “tumour” and “heart” can feel overwhelming.
The good news is this:
• Cardiac myxomas are benign (non-cancerous)
• In expert hands, surgical removal is highly effective and usually curative
• With modern keyhole (minimally invasive) heart surgery, recovery can be far quicker and less painful than many people expect
At The Keyhole Heart Clinic in London, my team and I regularly see patients who have been diagnosed with a cardiac myxoma – often “incidentally” on a scan done for something else – and are suddenly faced with the prospect of open-heart surgery. My goal in this article is simple:
To explain what a cardiac myxoma is, why surgery is almost always recommended, and how a keyhole approach can help you get back to normal life with less pain, fewer complications, and a faster recovery.
What is a cardiac myxoma?
A cardiac myxoma is the most common type of primary heart tumour in adults. “Primary” means it starts in the heart itself, as opposed to spreading from somewhere else in the body. Most myxomas are:
• Benign – they don’t behave like cancers and don’t usually spread to other organs
• Gelatinous and soft in texture
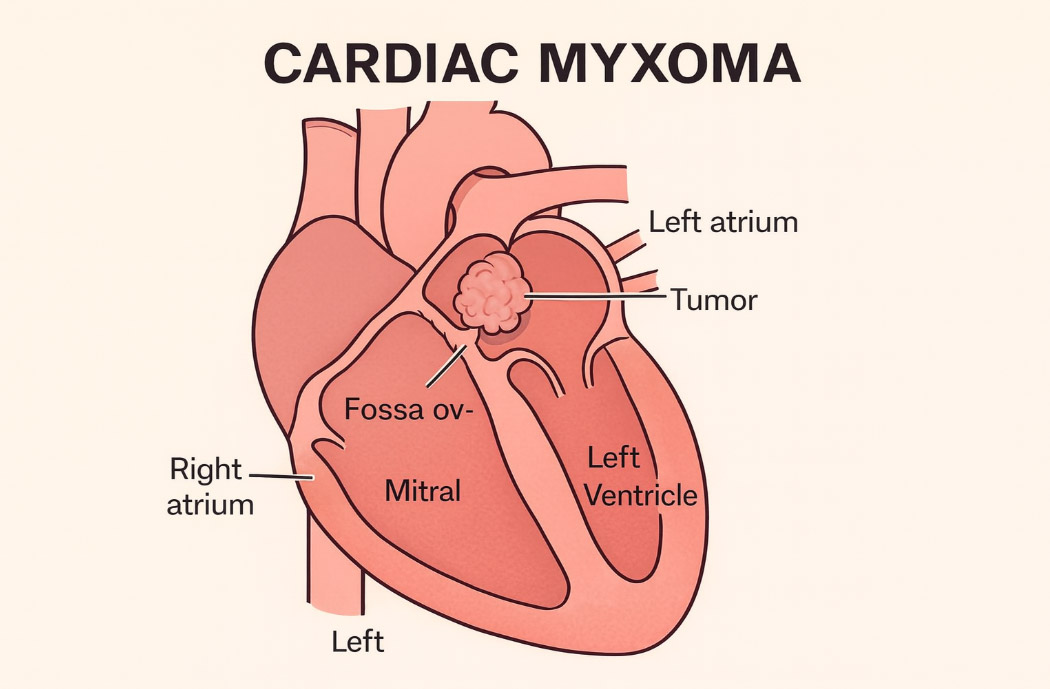
• Attached by a stalk to the inner wall of the heart, most often in the left atrium (the upper left chamber of the heart) near the mitral valve
Even though they are benign, they can still be dangerous because of where they sit and how they behave inside the heart.
How and where do they form?
Around 75% of cardiac myxomas arise in the left atrium, most of the rest in the right atrium; a smaller number occur in the ventricles. They tend to grow from the interatrial septum (the wall between the two upper chambers of the heart).
They are more common in:
• Adults between 30–60 years
• Women slightly more than men
• Occasionally, people with certain familial/genetic syndromes (for example Carney complex), where multiple tumours and other endocrine features may be present
Why can a benign tumour be so serious?
The key issue with a cardiac myxoma is not malignancy – it’s mechanics and embolisation.
1. Obstruction to blood flow
A myxoma often behaves like a ball-valve:
• As the heart beats, the tumour can swing into the mitral valve opening (or tricuspid valve if on the right side)
• It can partially or intermittently block blood flow, a bit like a plug being sucked into a drain
• This can cause breathlessness, dizziness, fainting, chest tightness, or even sudden collapse
Patients are sometimes misdiagnosed with mitral valve disease or heart failure before the tumour is found on an echocardiogram.
2. Risk of embolisation (bits breaking off)
Because myxomas are soft and friable, small fragments can break off and travel in the bloodstream (embolise).
If the tumour is in the left atrium, fragments can travel:
• To the brain → causing a stroke or transient ischaemic attack (TIA)
• To other organs (kidneys, spleen, limbs) → causing pain, organ damage, or limb ischaemia
Right-sided myxomas can send fragments to the lungs, causing pulmonary emboli and breathlessness.
3. Other symptoms
Some patients experience more general symptoms, including:
• Fatigue and low energy
• Weight loss
• Fever or night sweats
• Joint pains
These are thought to be due to inflammatory substances released by the tumour.
How is a cardiac myxoma diagnosed?
Most myxomas are picked up on imaging. Typical steps include:
Echocardiogram (heart ultrasound)
This is usually the first and most important test.
• Transthoracic echo (TTE) – ultrasound probe on the chest
• Transoesophageal echo (TOE/TEE) – ultrasound probe placed in the oesophagus to give a much clearer view
On echo, a myxoma looks like a mobile mass attached to the atrial wall, often wobbling with each heartbeat.
CT or MRI scan
Cardiac CT or MRI can:
• Confirm the size, location, and attachment point of the tumour
• Assess surrounding structures and help with surgical planning
Other tests
Depending on your symptoms, we may also arrange:
• ECG
• Blood tests
• Occasionally, additional imaging to look for embolic complications
Once a myxoma has been confirmed, the key question becomes: what next?
Do all cardiac myxomas need treatment?
In almost all cases, the answer is yes – they should be removed.
Even if you feel well, the risks of obstruction, stroke, or sudden collapse are unpredictable. These tumours do not shrink or disappear on their own. The longer they are left, the more opportunity there is for complications to occur.
International experience and published series over several decades consistently support early surgical removal once a myxoma is diagnosed, especially for tumours in the left atrium.
There are very few circumstances where surgery might be deferred – for example in very frail patients with multiple other serious conditions – but this is the exception, not the rule.
Treatment options: why surgery is the gold standard
There is currently no medication, radiotherapy, or catheter-based technique that reliably cures a cardiac myxoma.
The only definitive treatment is surgical excision:
-
Open the heart
-
Remove the tumour completely
-
Excise the base where it attaches (to reduce the risk of regrowth)
-
Repair the atrial wall and ensure the valves and chambers are functioning normally
Once removed completely, recurrence is uncommon, especially in non-familial cases. Long-term survival after surgery is usually excellent when the operation is performed before major complications occur.
The main choice is how the surgery is performed:
• Traditional sternotomy (splitting the breastbone)
• Modern keyhole (minimally invasive) approaches like those we specialise in at The Keyhole Heart Clinic
Traditional approach: sternotomy
For many decades, cardiac myxomas have been removed through a median sternotomy:
• A vertical incision is made down the centre of the chest
• The breastbone (sternum) is divided
• The heart is accessed directly
• The patient is placed on a heart–lung machine while the tumour is excised
This approach is effective and familiar to most cardiac surgeons. However, it comes with some drawbacks:
• More trauma – the breastbone is broken and needs time to heal
• More pain and discomfort in the early weeks
• Longer recovery – heavy lifting, driving, and certain movements are restricted while the bone heals (often ~6–12 weeks)
• Risk of sternal complications – infection, non-union, or chronic pain, especially in patients with diabetes, obesity, or osteoporosis
A different way: keyhole surgery for cardiac myxoma
At The Keyhole Heart Clinic, we specialise in minimally invasive, keyhole approaches to complex cardiac surgery – including tumour removal.
Instead of splitting the breastbone, we typically use a small incision between the ribs on the right side of the chest (a right mini-thoracotomy):
• The incision is usually 5–7 cm
• The ribs are gently spaced, not broken
• Specialised long instruments and high-definition cameras are used to work inside the heart
• The operation is still performed on a heart–lung machine, but access to the heart is through the side of the chest rather than through the sternum
The tumour is then removed under direct vision, along with a small cuff of tissue at its attachment point. The atrial wall is repaired, and the valve function is carefully checked.
Why keyhole makes such a difference
Because we avoid breaking the breastbone, patients usually experience:
• Less pain
• Smaller scars – often hidden under the breast in women
• Earlier mobilisation – walking and moving freely much sooner
• No need for the long list of sternal movement restrictions (no pushing trolleys, no lifting heavy objects, no driving for several weeks, etc.)
• A quicker return to normal daily life, work, and exercise
Many of our patients are independently mobile, climbing stairs, and performing basic self-care within days. While everyone heals at their own pace, the difference between recovering from a broken breastbone and a keyhole incision between the ribs is profound.
From a surgical perspective, in experienced hands, keyhole approaches allow:
• Excellent visualisation of the tumour and its attachment
• Safe and complete excision
• The ability to address any associated valve problems at the same sitting (for example, repairing the mitral valve if needed)
What happens before, during, and after keyhole myxoma surgery?
1. Pre-operative assessment
At The Keyhole Heart Clinic, we start with a comprehensive review:
• Detailed history and examination
• Review of your echocardiogram, CT or MRI scans
• Assessment of your general health, lungs, and other organs
• Multidisciplinary discussion between surgeon, cardiologist, and anaesthetist
We will talk through:
• The nature of the tumour and its risks
• Your personalised surgical plan
• Whether a keyhole approach is suitable for your specific anatomy and medical condition
• The likely recovery timeline and follow-up
Our aim is for you to feel fully informed and confident before you make any decision.
2. The operation
On the day of surgery:
-
You receive a general anaesthetic and are fully asleep
-
A small incision is made on the right side of the chest, between the ribs
-
The heart is connected to a heart–lung machine
-
The appropriate chamber (usually the left atrium) is opened
-
The myxoma is inspected and carefully removed
-
The atrial wall and any affected valve structures are repaired
-
The heart is closed and normal circulation restored
The surgical time is dependent on the complexity of the case, but from your perspective, the key point is that you are comfortable and closely monitored throughout.
3. Recovery in hospital
After surgery:
• You’ll spend a short time in the intensive care or high dependency unit
• Most patients are sitting up and walking with help within 24–48 hours
• Pain is managed proactively – often described as tightness or ache rather than severe pain
• We’ll encourage breathing exercises and physiotherapy to prevent stiffness and help your lungs expand fully
Our team is highly experienced at guiding patients through this early phase, and our focus is always on safe, confident mobilisation as soon as possible.
4. Recovery at home
Once home, patients recovering from keyhole surgery generally notice:
• They can use their arms normally – turning in bed, getting out of a chair, opening doors, even light housework, much earlier than after sternotomy
• They are able to walk several times per day, gradually increasing distance
• There is no sense of “bone movement”, which many sternotomy patients describe in the first few weeks
Return to office-based work is often possible within a few weeks, though this varies by individual and by the demands of your job. More physical jobs may take longer, but again, the absence of a broken breastbone makes a substantial difference.
We’ll see you in follow-up, usually with a repeat echocardiogram, to confirm:
• The tumour has been completely removed
• The valves and heart function are satisfactory
• You’re progressing well with your recovery and rehabilitation
Is keyhole surgery suitable for everyone with a cardiac myxoma?
Keyhole techniques are powerful tools, but they are not “one-size-fits-all”.
Suitability depends on:
• Tumour location and size
• Your body shape and chest anatomy
• Previous heart or chest surgery
• Other heart conditions that might need to be addressed at the same time
In many patients, particularly those with left atrial myxomas, a keyhole approach is not only feasible but highly advantageous. In others, a more traditional approach may still be the safest option.
The most important thing is that your case is assessed by a team with extensive experience in both conventional and keyhole methods, so the recommendation you receive is based on what is truly best for you – not what happens to be the only technique available locally.
At The Keyhole Heart Clinic, my team and I are known for our work in advanced minimally invasive cardiac surgery. When we meet patients with a myxoma, we look very carefully at whether a keyhole approach can be safely offered, and we will explain our reasoning in plain language.
What are the risks of surgery?
All heart surgery carries some risks. Common risks include:
• Bleeding
• Infection
• Stroke or other embolic events
• Heart rhythm problems (e.g. atrial fibrillation)
• Complications from anaesthesia or other medical conditions
Risk is often favourable when:
• The tumour is treated before major complications occur
• You are otherwise fit and well
• Surgery is performed in a specialised centre
With keyhole approaches, the risk to life and major organ function is typically comparable to conventional surgery in suitable patients, but with the added benefits of less trauma and faster recovery.
During your consultation, we will go through your personalised risk profile in detail and answer all your questions.
Life after myxoma surgery: what to expect
For most patients:
• The tumour does not return (especially in non-familial cases)
• Symptoms like dizziness or breathlessness usually resolve
• Long-term prognosis is excellent
You may need:
• Follow-up echocardiogram at intervals
• Ongoing care for any other cardiac issues you might have (for example: blood pressure, arrhythmias, or coronary disease)
But in terms of the myxoma itself, the operation is generally curative.
From a lifestyle perspective, especially after keyhole surgery:
• Return to exercise and sport is often possible once cleared
• Travel and a full, active life is achievable
• Often tell us that, after the initial shock of diagnosis, they feel they’ve been given a “reset” and are more motivated than ever to look after their heart health going forward
Why choose The Keyhole Heart Clinic?
You might be:
• Worried that only full sternotomy is being offered
• Unsure whether keyhole options exist in the UK
• Seeking a second opinion from an experienced team
At The Keyhole Heart Clinic, we work around three core principles:
1. World-class surgical expertise
• My practice is dedicated to minimally invasive and keyhole heart surgery, including complex valve and coronary procedures as well as tumour surgery.
• We work within established UK hospital environments with full intensive care support and multidisciplinary input.
2. Personalised, honest advice
• We will tell you clearly and transparently whether a keyhole approach is suitable in your case.
• If we believe keyhole is not in your best interests, we will explain why and outline the safest path forward.
3. Faster, kinder recovery
• Our focus is not just on removing the tumour, but on how quickly and comfortably you can get your life back.
• That means meticulous surgery, but also excellent anaesthetic care, physiotherapy, rehabilitation, and follow-up.
Final thoughts
Being told you have a cardiac myxoma can be frightening, but in expert hands, we can often say something reassuring:
We know what this is. We know how to fix it. And in most cases, surgery offers an excellent chance of a complete cure.
If you or someone you love has been diagnosed with a cardiac myxoma and you’ve been told that only traditional open-heart surgery is possible, you are very welcome to seek a specialist keyhole opinion.
Whether or not keyhole surgery turns out to be right for you, you deserve to understand all your options, to ask questions in language you can understand, and to feel you are in the hands of a team that does this kind of complex work every day.
If you’d like to explore whether a minimally invasive, keyhole approach to myxoma removal is suitable in your case, my team at The Keyhole Heart Clinic would be delighted to help.

